Breast Lumpectomy Surgery by PecsBlock Without General Anesthesia
Ida Bagus Reza Nanda Iswara, Wayan Widana
Ida Bagus Reza Nanda Iswara, Wayan Widana

Breast Lumpectomy Surgery by PecsBlock Without General Anesthesia
Sumber: Medicinus April 2021 vol. 34 issue 1
Ida Bagus Reza Nanda Iswara, Wayan Widana
Departement of Anesthesiology & Pain Medicine Wangaya Hospital Denpasar
Abstract
Breast conserving surgery is usually performed under general anesthesia, or more recently combined with regional anesthesia techniques. Thoracic spinal block, thoracic epidural block, and thoracic paravertebral block are options of regional anesthesia that have been used in breast surgery, but anesthesiologists avoid them due to concern in potency of complications and side effects. After introduced by Blanco in 2011, pectoral nerves (Pecs) block appears as alternative procedure with fewer complications and lower incidence of postoperative pain. In this case report we describe a 32-year-old female patient admitted for elective lumpectomy of the left upper quadrant of the breast. Ultrasound guided Pecs II block was chosen as the anesthetic technique for this patient.
The authors reported successful management of anesthesia and pain without complications in breast surgery. Pecs II block as single anesthetic technique can be considered safe, advantageous, and effective in breast surgery with good hemodinamic stability and low inicidence of side effects.
Introduction
Breast cancer is the most common cause of malignant neoplasm in women. In Indonesia, breast cancer contributes for more than 30% of all malignancies, and its’ incidence has increased significantly in the last decades. Surgery is the treatment of choice for this kind of cancer, and it is usually performed under general anesthesia. Recently, combined regional and general anesthesia technique becomes common in the management for breast cancer surgery. Thoracic paravertebral block (TPVB), thoracic epidural, and thoracic spinal block were initially the standard of choices, despite the complications and technical difficulties.1
In 2012, Blanco introduced pectoral nerve (Pecs) II block or modified Pecs block as a novel approach to breast surgery. This new approach aims to provide effective anesthesia and multimodal postoperative analgesia in breast surgery. Several studies reported its’ advantages as combined anesthetic technique with general anesthesia, but only a few use it as single anesthetic technique. Pecs II block is technically simple, easy to perform, with lower risk of complications. Regional anesthesia technique also offers reduction in postoperative pain and postoperative nausea and vomiting (PONV).2.
Case Report
A 32-year-old woman (163 cm, 60 kg) came to Wangaya Hospital with abcess and mass in her left breast that was identified by the ultrasound imaging (Fig. 1). Patient was diagnosed with left breast tumor suspect invasive ductal carcinoma. She had no medical history and scheduled for lumpectomy and biopsy. Ultrasound guided Pecs II block was considered as the anesthesia technique for this surgery. ASA standard monitoring was placed (blood pressure monitor, pulse oxymetri, electrocardiogram), and patient was given premedication with 2 mg of intravenous midazolam. Patient positioned in a supine position with abduction 90o of left arm. Supplemental oxygen was provided by nasal cannule (4 L/min). The left breast and axillary regions were cleaned using iodine. Under aseptic condition, ultrasound probe was placed under the lateral third of the left clavicula, identifiying the third and fourth ribs. Local anesthetic with 2% lidocaine was infiltrated at the puncture site.
For the first injection, a 22-gauge needle was inserted, placed between the pectoralis minor and major muscle, injecting 10 ml of 0.25% bupivacaine (Fig. 2A). Hydrosection was observed between both muscle, blocking the medial and lateral pectoral nerves. The second injection was made between the pectoralis minor and serratus anterior muscle, injecting 20 ml of 0.25% bupivacaine with intention of blocking long thoracic, thoracic intercostal T2-T6 and thoracodorsal nerves (Fig. 2B). This Pecs II block procedure took about 15 minutes and onset time of analgesia was 15 minutes after completion, confirmed by pinprick test.
Hemodynamic stability was maintained during the entire procedure (50 minutes), referring the patient to the postanesthesia care unit without additional analgesic or antiemetic drugs. Patient did not complain about postoperative pain of the surgical site 8 hours after surgery. VAS score 8 hours after surgery was 0/10.
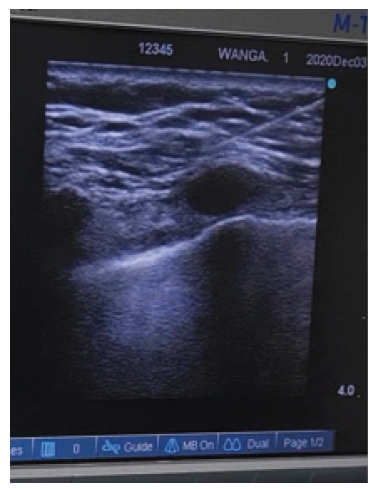
Figure 1. Ultrasound imaging 1.07 x 1.08 cm and 0.5 x 0.7 cm multiple hypoechoic mass on left breast
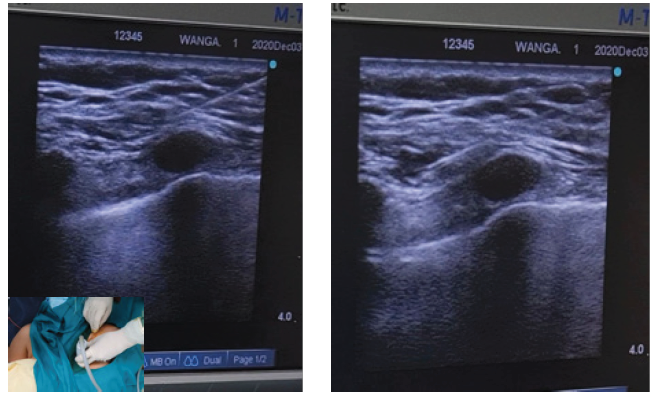
Figure 2. The 22-gauge needle was placed between pectoralis major and minor muscle for the first injection with 10 ml of 0.25% bupivacaine (A), then advanced to fascia between pectoralis minor and serratus anterior muscle, injecting 20 ml of 0.25% bupivacaine (B)
Discussion
Breast surgery is associated with acute and severe postoperative pain, as well as restriction of arm mobility. In this case report, Pecs block is described as a simple and effective technique in perioperative analgesia for breast cancer surgery, as an alternative to conventional regional anesthesia such as thoracic spinal block, thoracic epidural, and thoracic paravertebral block (TPVB). Regional anesthesia has some benefits in reducing postoperative pain and postoperative nausea & vomiting (PONV) by decreasing the opiate use, thus lowering side effect for breast surgery patient compared to general anesthesia. TPVB is currently the gold standard for the regional anesthesia in breast surgery. Kulhari and Bharti found that patients that undergo Pecs block have longer duration of analgesia compared to thoracic paraverterbral block, lowering opioid consumption during first 24 hour. This ultrasound guided Pecs block is technically simpler, faster, high success rate, with lower risk of complications, which make it as an excellent alternative to conventional regional techniques or general anesthesia for breast surgery.4
Pecs I block was introduced in 2011 by Blanco as interfascial block of the lateral and medial pectoral nerve, performed by hydrodissection of the plane between pectoralis minor and major muscle with local anesthetic. The main landmarks to identify the point of injection are the pectoralis major and minor muscle and the pectoral branch of the thoracoabdominal artery. Patient is positioned in supine position with arm next to chest or abducted 90 degrees. The suggested volume is 0.2 ml/kg of long-acting local anesthetic, and proper fascial plane is confirmed by hydrodissection of this local anesthetic to open the space between the pectoralis muscle.2
Later in 2012, Blanco introduced the Pecs II block or modified Pecs block. Pecs II added the long thoracic nerve, thoracic intercostal nerve from T2-T6, and thoracodorsal nerve, hence providing analgesia in more extensive surgeries such as tumor resection, sentinel node biopsy, and mastectomies. This block consist of two injections. The first injection is the same as Pecs I block, while the second injection is made at the anterior axillary line at the level of the fourth ribs. Here is where the 0.2 ml/kg of long-acting local anesthetic injected to hydrodissected space between the pectoralis minor and serratus anterior muscle.3
Most cases of Pecs block are performed under general anesthesia (GA) for postoperative pain management. Senapathi, et al. (2019) and Bashandy, et al. (2015) conducted randomized clinical trial with 2 groups that consist of GA alone group and combined GA with Pecs block group. Pecs group showed significantly lower intraoperative opioid consumption, lower VAS score, and lower 24-hours postoperative opioid consumption without any complications.5,6
A single regional anesthetic technique also can be used in breast surgery. Hakim and Wahba (2019) conducted a randomized clinical trial using Pecs block versus local anesthetic infiltration, with Pecs group showed lower VAS and total morphine consumption after surgery. Study comparing Pecs II to TPVB by Wahba and Kamal (2014) concluded that Pecs II reduces postoperative opioid consumption and better pain relief compared to TPVB. Eldeen (2016) found that Pecs II block and thoracic spinal block (TSB) provide effective intraoperative anesthesia and postoperative pain relief, but Pecs II is relatively simpler and safer.7,8,9
Although the Pecs block is considered safe, there is still possibility to puncture the artery between the pectoralis major, minor, and serratus anterior muscle. Artery puncture and hematoma maybe one of the risk of this procedure.1,4
In conclusion, the Pecs block can be helpful in patient undergoing simple breast surgery or in high-risk patient for general anesthesia. Pecs II block as single anesthetic technique may be safe and advantageous alternative which provide sensory block with good hemodynamic stability and low inicidence of side effects. Pecs II block also reduces the postoperative pain, postoperative opioid consumption, and PONV incident.
Conflicts of Interest
No potential conflicts of interest relevant to this article was reported
DAFTAR PUSTAKA